


How Long Does Gabapentin Last in Dogs? A Veterinarian's Clinical Guide

Gabapentin lasts approximately 6 to 8 hours in dogs with normal kidney function. The plasma half-life is 3 to 4 hours, which translates clinically to that 6–8 hour analgesic or anxiolytic window per dose. Outside that window, plasma concentrations drop below the range associated with meaningful pain control or seizure suppression.
That single pharmacokinetic fact carries more practical weight than almost any other gabapentin consideration in small animal medicine — it determines the dosing interval, sets owner expectations, and is the most common reason pain protocols underperform when written incorrectly.
What the Pharmacokinetic Data Actually Says
Oral bioavailability in dogs sits around 80%, based on pharmacokinetic data from KuKanich and Coetzee (Journal of Veterinary Pharmacology and Therapeutics, 2011). Peak plasma concentration arrives within 1 to 2 hours of an oral dose, and the decline after that is consistent: by hour 6 or 7, most healthy dogs are at subtherapeutic concentrations.
Absorption is not meaningfully affected by food, which is worth mentioning to owners — no empty-stomach requirement, no timing around meals, one less variable in the discharge routine.
Dr. Sheilah Robertson, BVMS, PhD, DACVAA, DECVAA, a board-certified veterinary anesthesiologist whose published work covers multimodal analgesia in companion animals, has noted that dogs metabolize gabapentin faster than humans and that bioavailability varies more between individual patients than practitioners often expect. The source of that variability is not breed or body weight — it is renal function.
Gabapentin clears through the kidneys, not the liver. It bypasses cytochrome P450 entirely, which is why it does not affect phenobarbital metabolism the way many other anticonvulsants do. A dog with a creatinine of 3.5 holds gabapentin in circulation far longer than a healthy dog of the same weight on the same dose.
Give the renally compromised patient the standard mg/kg dose, and you risk oversedation with an amount that would be unremarkable in a different animal.
Older dogs are where this risk is greatest. Creatinine is a late marker — renal function must decline by roughly 66–75% before serum creatinine rises above the normal reference interval. SDMA picks up GFR decline earlier, sometimes by months to years.
A geriatric dog with a clean creatinine can still carry SDMA values that change how gabapentin behaves. Starting this drug in a 12-year-old Cavalier without an SDMA is taking an avoidable guess. For a deeper look at monitoring renal biomarkers in aging dogs, see our companion article on chronic kidney disease in dogs.
Critical Formulation Warning: Human liquid gabapentin preparations — including compounded versions — may contain xylitol as a sweetener. Xylitol is acutely toxic to dogs, causing rapid insulin release and potentially fatal hypoglycemia. Always verify the formulation before dispensing or approving a refill. Dog-safe liquid preparations must come from a veterinary compounding pharmacy using xylitol-free excipients. Capsules and tablets do not carry this risk, but always confirm ingredients when a human-labeled product is involved.
How Long Does Gabapentin Last for Each Condition?
Postoperative and Neuropathic Pain
Published analgesic dosing sits at 5 to 10 mg/kg every 8 hours for postoperative pain. Dogs prescribed gabapentin on a twice-daily schedule for surgical recovery are going without meaningful plasma levels for several hours of every 24-hour period. Discharge instructions should be specific: every 8 hours means every 8 hours, not two to three times a day.
For neuropathic pain, some specialists push doses above the standard range. Dr. Loïc Dobenecker, veterinary pharmacologist at Ludwig Maximilian University (LMU) Munich, noted in a 2020 clinical review that neuropathic pain in dogs often requires doses beyond what older small animal references recommend — partly because neuropathic pain responds poorly compared to nociceptive pain, and partly because the ceiling effect of gabapentin in dogs is not well characterized.
A dog that can barely lift its head is not a dog whose pain is controlled. It is a dog that is drowsy. Discharge instructions must say this clearly. 'Calm and resting' is appropriate. 'Won't respond to its name' is not.
Unlike NSAIDs such as carprofen, meloxicam, deracoxib, or firocoxib — which carry gastrointestinal and renal risks from their mechanism of action — gabapentin does not produce organ toxicity at therapeutic doses. That said, it still requires renal monitoring because impaired clearance changes how long it stays active.
When NSAIDs are contraindicated in CKD patients, gabapentin is frequently part of the analgesic plan, sometimes alongside tramadol or opioids, with dose adjustment for renal function.
Seizure Management
Gabapentin in epileptic dogs functions as an add-on drug, typically alongside phenobarbital or potassium bromide. It is not used as a sole anticonvulsant. Dosing for seizure control runs every 6 to 8 hours; some neurologists extend to every 8 to 12 hours in closely monitored patients using seizure diaries.
The 2017 Govendir et al. study (Australian Veterinary Journal) found that adjunctive gabapentin cut seizure frequency by more than 50% in 58% of dogs studied. The same study noted that therapeutic drug monitoring for gabapentin is not standardized in veterinary medicine. In human neurology, plasma gabapentin levels are checked routinely. In dogs, dosing remains empirical: adjust based on seizure frequency and adverse effects, not a target plasma concentration. Phenobarbital metabolism, notably, is unaffected by gabapentin because neither drug touches the CYP450 pathway.
Stopping gabapentin in a dog on long-term seizure management requires a taper, not an abrupt discontinuation. Most neurologists use 2 to 4 weeks when discontinuing after extended use. Abrupt cessation after prolonged therapy raises the risk of rebound seizure activity — the mechanism mirrors what occurs in human neurology patients.
Situational Anxiety
For noise phobia, vet visit anxiety, or fireworks, the most widely used protocol is 20 mg/kg given 1 to 2 hours before the stressor. Anxiolytic effect aligns with the analgesic window — approximately 6 to 8 hours — with residual sedation that runs longer in some patients. For this indication, a single dose is appropriate and the evidence supports it.
Unlike the pain or seizure indications, once-daily dosing is clinically justified here because it corresponds to a single, defined event.
Gabapentin Dosing Reference by Indication
Dosing drawn from published veterinary pharmacokinetic and clinical literature. Adjust to individual patient response and renal function.
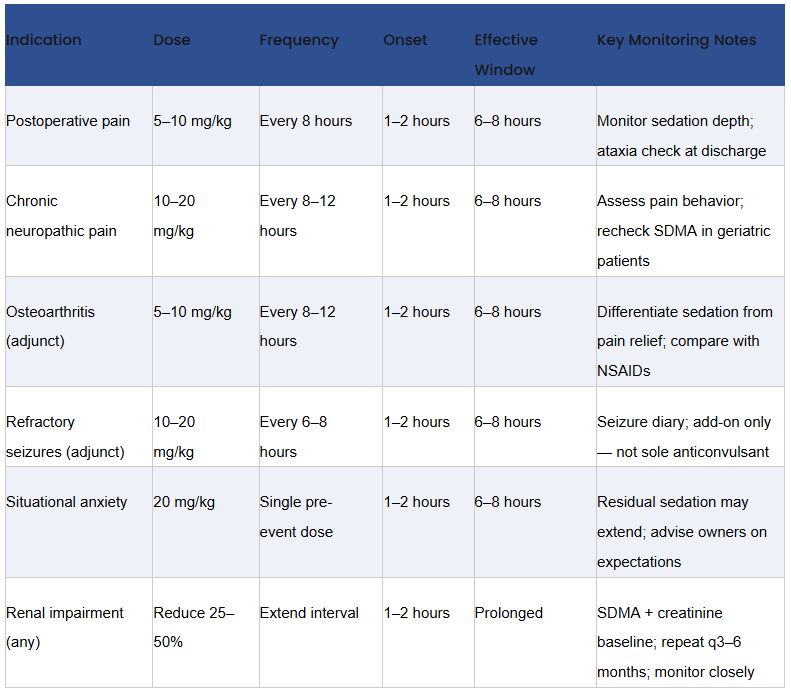
Note: All doses are off-label in veterinary medicine. Renal impairment cases should have SDMA and creatinine established before initiating therapy and repeated every 3–6 months during treatment.
Drug Interactions: What to Know Before Combining Gabapentin
Any CNS-active medication adds to gabapentin's sedative effect. Opioids, acepromazine, trazodone, alprazolam, and benzodiazepines all interact additively. Combining them is not wrong — multimodal analgesia protocols routinely include gabapentin alongside one or more of these — but owners going home with a dog on multiple sedating drugs need an explicit conversation about what normal looks like and what crosses the line into a callback situation. Leaving that vague produces unnecessary emergency contacts and missed early warning signs.
Aluminum- or magnesium-based antacids administered concurrently can reduce gabapentin absorption. Timing those medications separately by at least 2 hours is reasonable practice if antacids are part of the patient's protocol.
Gabapentin has no interaction with phenobarbital pharmacokinetics, which is one of the reasons it became a practical adjunct in refractory epilepsy — it does not alter existing drug levels in polypharmacy patients.
Tramadol, often discussed alongside gabapentin in multimodal pain protocols, warrants a note: multiple studies in dogs have found tramadol to be ineffective for osteoarthritis pain, and its mu-opioid activity in dogs is considerably lower than in humans due to differences in CYP2D6 metabolism.
When codeine-based preparations are used, monitoring for sedation is appropriate, particularly in combination with gabapentin. Carprofen and other NSAIDs remain first-line for OA in dogs with adequate renal function, with gabapentin as an adjunct for neuropathic or central sensitization components.
What Makes the Duration Shorter or Longer in Individual Dogs?
Kidney function drives more individual variation than any other factor. A dog with advancing CKD is not just a sick patient who needs a lower dose; their clearance rate has changed enough to alter when the next dose should happen, not just how much. Dose reductions of 25–50% with extended intervals are appropriate starting points, adjusted based on response and follow-up renal values.
Among geriatric patients, GFR decline often goes undetected by creatinine alone. SDMA begins signaling earlier — detecting approximately 25% GFR loss, compared to the 60–75% loss required before creatinine becomes abnormal. Running an SDMA before initiating gabapentin in any dog over 8 to 10 years old is a reasonable standard, not an optional add-on.
Long-term tolerance is a concern owners often raise after reading about opioid tolerance, assuming the same pattern applies. The veterinary data on gabapentin tolerance in dogs is limited, but clinical experience with long-term osteoarthritis patients does not show the same escalating dose requirement seen with opioids. This does not mean tolerance never occurs; it means the evidence for it is thin and should not drive premature dose escalation.
When Gabapentin Stops Controlling the Problem
The most common reason is that the dosing interval is too long. A dog with neuropathic pain dosed every 12 hours is getting roughly 8 hours of coverage and 4 hours of inadequate plasma levels per cycle — that gap accumulates. Before switching drugs or adding a new agent, tighten the interval and reassess at the next visit.
If the interval is already appropriate and the response is poor, the dose may need to go up, or the condition has moved beyond what gabapentin alone can address. Neither scenario is a reason to abandon the drug — it is a reason to consider what else the protocol needs, whether that is a dose adjustment, an NSAID where appropriate, or a referral for further pain workup.
In seizure patients, a cluster of activity near the end of a dosing interval is a signal that the interval is too long for that individual dog. The solution is usually shortening the interval or adding a second adjunctive agent, not switching primary anticonvulsants — especially in patients with established phenobarbital or potassium bromide levels.
What Vet Techs Should Be Checking at Rechecks
Before the veterinarian sees the dog, collect three pieces of owner-reported information: whether the dog is eating normally, whether the dog seems more sedated than expected, and whether any stumbling or coordination difficulty has been noticed. Ataxia is the one that is most often missed in disc disease or spinal pain patients. A dog that looks neurologically worse after starting gabapentin may not be deteriorating — it may simply be overmedicated. Catching that observation before the exam saves an unnecessary workup and reframes the clinical picture correctly.
Bloodwork every 3 to 6 months is appropriate for dogs on gabapentin chronically. The target is renal function — creatinine and SDMA — not a gabapentin plasma level. There is no standardized therapeutic window in veterinary patients the way there is for phenobarbital. Dose decisions remain clinical: owner-reported behavior, in-clinic observation, and serial renal values are doing the work that therapeutic drug monitoring handles in human neurology.
For vet techs looking to build deeper pharmacology skills around analgesic protocols and CNS-active drugs,Vet and Tech's free RACE-approved CE webinars cover pain management, seizure care, and other clinical topics directly relevant to this area of practice.
Gabapentin is also widely used in feline patients, but the pharmacokinetics differ from dogs in ways that affect dosing and duration. If you work with cats as well, see our detailed guide: How Long Does Gabapentin Last in Cats?
Frequently Asked Questions
How long does gabapentin last in dogs after a single dose?
Gabapentin lasts approximately 6 to 8 hours in a dog with normal kidney function. Peak plasma concentration is reached within 1 to 2 hours of an oral dose. By hour 6 to 7, most healthy dogs are below the therapeutic range. In dogs with renal compromise, that window extends because clearance slows — sometimes considerably, depending on the degree of dysfunction.
Can you give gabapentin to a dog once a day?
For pain or seizures, no. The half-life does not support once-daily dosing — it results in many hours per day with no meaningful plasma levels. The one exception is situational anxiety: a single 20 mg/kg dose given 1 to 2 hours before a specific stressor is appropriate and well-supported. Any other indication requires at minimum twice-daily, and ideally three-times-daily dosing.
Does kidney disease change how long gabapentin stays active in dogs?
Yes, and it matters more than any other individual variable. Because renal clearance is the primary elimination route, any reduction in kidney function extends gabapentin's duration and raises the risk of accumulation and oversedation. CKD patients should start at 25–50% lower doses with extended intervals, adjusted to clinical response. SDMA is preferable to creatinine alone as the monitoring biomarker.
What does gabapentin wearing off look like in a dog?
Pain behaviors return: vocalizing, reluctance to move, changes in posture, reduced appetite, social withdrawal, or restlessness. In seizure patients, clustering near the end of a dosing interval is a reliable clinical signal that the interval is too long for that individual. These patterns should be explicitly included in owner discharge education — they are the behavioral equivalent of drug-level monitoring.
Is gabapentin safe for long-term use in dogs?
For dogs with stable or adequately monitored kidney function, long-term use is considered clinically safe. Bloodwork every 3 to 6 months is warranted to track renal function. Dogs on gabapentin for seizure control for more than 4 to 6 weeks should be tapered rather than stopped abruptly if discontinuation is planned, to reduce the risk of rebound seizure activity.
What drugs interact with gabapentin in dogs?
Any CNS depressant — opioids, acepromazine, trazodone, alprazolam, and benzodiazepines — will produce additive sedation when combined with gabapentin. Owners need explicit guidance on expected sedation levels. Aluminum- or magnesium-containing antacids may reduce gabapentin absorption if administered simultaneously; spacing them by 2 hours is recommended. Gabapentin does not interact with CYP450-metabolized drugs, so phenobarbital, NSAIDs such as carprofen, meloxicam, and deracoxib, and most other common veterinary medications are unaffected pharmacokinetically.
Is human liquid gabapentin safe for dogs?
Not necessarily. Many human liquid formulations of gabapentin contain xylitol, which is toxic to dogs and can cause life-threatening hypoglycemia. Liquid gabapentin for dogs must come from a veterinary compounding pharmacy that uses xylitol-free formulations. Always verify the ingredient list before dispensing any human-labeled liquid preparation, and advise clients never to use human oral solutions without veterinary confirmation.
Sources and Further Reading
1. KuKanich B, Coetzee JF. Opioids in veterinary medicine — gabapentin pharmacokinetics in dogs. Journal of Veterinary Pharmacology and Therapeutics. 2011.
2. Govendir M, Perkins M, Malik R. Improving seizure control in dogs with refractory epilepsy using gabapentin as an adjunctive agent. Australian Veterinary Journal. 2005;83(10):602–608. [Note: Verify current indexing edition with your institution — confirm against PubMed before citing in clinical materials.]
3. Dobenecker L. Gabapentin dosing in neuropathic pain in dogs: clinical pharmacology review. Ludwig Maximilian University Munich, Faculty of Veterinary Medicine. 2020 clinical review.
4. Robertson SA. Multimodal analgesia in companion animals. Published clinical and conference proceedings, including DACVAA/DECVAA-affiliated continuing education materials.
5. Vet and Tech. How Long Does Gabapentin Last in Cats? vetandtech.com/blogs/how-long-does-gabapentin-last-in-cats-insights-for-veterinarians
6. Vet and Tech. Types of Seizures in Dogs: Symptoms, Causes and Treatment Guide. vetandtech.com/blogs/types-of-seizures-in-dogs-symptoms-causes
7. Vet and Tech. Chronic Kidney Disease in Dogs — Early Identification and Monitoring. vetandtech.com/blogs
8. Vet and Tech. Free RACE-Approved Veterinary CE Webinars. vetandtech.com/blogs/elevate-your-skills-free-veterinary-ce-online-opportunities-await
9. IRIS (International Renal Interest Society) Staging System for CKD. iris-kidney.com
10. Today's Veterinary Practice. Multimodal Pain Management for Canine Osteoarthritis. todaysveterinarypractice.com
This article is intended for veterinary professionals. All dosing is off-label in veterinary medicine and should be adjusted based on individual patient assessment. Verify all citations against current indexed literature before use in formal clinical materials.




